Best of Kin
Healthcare

How We Relate Determines How Well We Can Run
Blended families are no longer the exception but increasingly the norm. While a beautiful expression of love, the family blend often adds a level of complexity to the logistics of busy, mobile lives. Same is true for integrated health systems. Most are a “blend” of hospitals, doctors and ambulatory sites which come to the “family” with their own culture, operating model and organizational DNA. Assimilating those lines under a common brand often scrubs some of the sharpest differences off the legacy operating models. But is assimilation enough?
For integrated health systems, the evidence suggests not. Most integrated health systems are still plagued with the reality of business lines working “alone, together” in one of two configurations.
In the first, the health system appropriately views customers through the lens of the master brand, yet still channels those customers through a thicket of disjointed and often sub-branded operating systems that disconnect from the family brand. This is frequently experienced as a station-to-station journey with repeat registration, disconnected scheduling and disparate billing systems.
In the second, integrated networks leverage shared systems to take the seams out of patient navigation. They operate with centralized scheduling, registration and billing platforms. Yet, internal, clinical lines persist in competing with one another for business and resources.
In both cases the perceptual promise of a “system whole” that exceeds the sum of the integrated parts is exposed as little more than increased overhead and added complexity that adds no new value to the customer. In both iterations, the root cause is not suboptimal operating performance within the lines, but parochialism across the lines. In short – the aggregated pieces and parts may all share the same surname but from a customer point of view act like anything but best of kin.
Self-Assessment
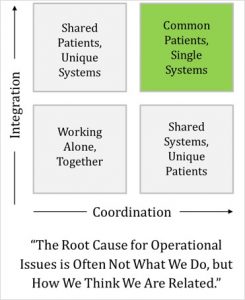
How does your system perform? Consider the two-by-two grid above, and decide which of the four boxes best describes the culture of your enterprise. To guide that assessment, consider the signs of an organization that is still in the lower left quadrant of “working alone, together.”
Five “Red Flags” of Working Alone, Together
- System leadership meetings are highly tactical, not about what make us distinctive
- Our marketing communications sounds like our competitors’ claims
- The leadership team frequently talks about the risk of cannibalizing hospital business
- Our strategic priority is stated as market share, not meeting customer needs and aspirations
- System IT teams have disproportionate influence over how fast we get products to market
Think about leaders and management in your organization. Most health systems presume that their managers are leaders – either because the role confers that authority on them or because leadership was thought to be a pre-cursor to getting a management role. That assumption is not only false, but it ignores the reality that managers and leaders have unique roles in leading organizations from the lower-left quadrant of working alone together to the upper-right quadrant of performing as a highly reliable, distinctive system of care.
In his Harvard Business Review article, “What Leaders Really Do”, the noted author John Kotter contrasted the unique roles of management and leadership. We believe these distinctions are critical.
Management
- Planning and budgeting
- Organizing and staffing
- Control and problem solving
Leadership
- Setting direction
- Aligning people
- Providing motivation
(Source: “What Leaders Really Do”, John Kotter, Harvard Business Review)
Assess your own senior leadership team. Is it clear to the people around the table whether they are expected to be managers or leaders? Is the team agenda organized around management purposes (we plan, budget, organize and staff), or leadership goals (we set direction, align and motivate people)? Answering those foundational questions can be a critical insight into changes you need to make as the executive leader in moving your organization from the underperforming lower-left quadrant to the market-driving upper right.
BVK Brand+Lever works with CEOs and senior executive teams to transform their business models to deliver distinctive, brand-driven service experiences. We see operations and leadership as critical dimensions of building strong brands. To learn more, or schedule a discussion with your leadership team, please contact Mike Eaton, BVK Brand+Lever Senior Vice President at [email protected].